When you think that of John Lennon of The Beatles, you most likely imagine him wearing round, wire-rimmed glasses.
But he did wear contacts sometimes, or not less than he tried to. They kept squeaking in his eyes.
What Lennon did, and why, to assist his contact lenses stay in place is part history, part vision science.
As I propose in my paperit also involved smoking large amounts of weed.
Lennon didn’t like wearing glasses.
Before 1967, Lennon rarely wore glasses in public. His aversion to wearing them began in childhood, when he was diagnosed with nearsightedness at around age 19. seven.
Nigel Walley was Lennon’s childhood friend and manager of The Quarrymen, the forerunner of The Beatles. Walley he told the BBC:
He was blind as a bat – he had glasses but never wore them. He was very vain about it.
In 1980, Lennon Rolling Stone said warehouse:
I spent my entire childhood without glasses because glasses were wimps to me.
Even during long tours Beatlemania (1963–66)Lennon, unlike his idol Buddy Holly, never wore glasses during live performances.
Then Lennon tried contact lenses… ping!
Roy Orbison’s guitarist Bobby Goldsboro introduced Lennon to contact lenses in 1963.
But Lennon’s foray into the world of contact lenses was relatively short-lived. The lenses kept falling out – even during filming a comedy sketch, on stage (when a fan threw jelly on stage and it hit him in the eye) and in the pool.
Why? It was probably a mixture of the lenses available at the time and the shape of Lennon’s eye.
Provided by the creator
The soft, flexible contact lenses that thousands and thousands of individuals wear today weren’t commercially available until 1971In the Sixties, only rigid contact lenses were available, of which there have been two types.
The large “scleral” lenses rested on the white of the eye (sclera). They were partially covered by the eyelids and rarely moved.
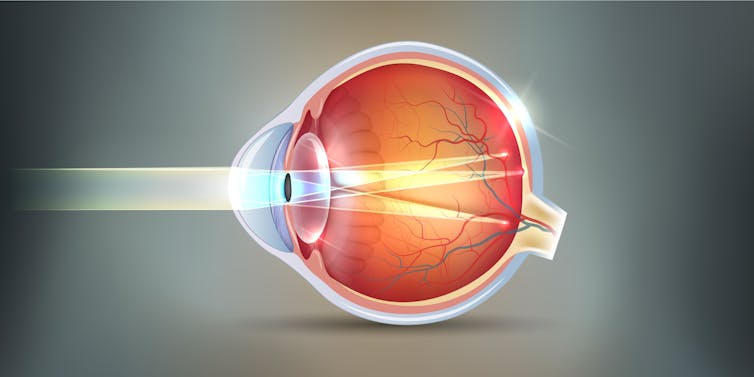
But the smaller “corneal” lenses rested on the front surface of the cornea (the outermost, clear layer of the eye). This was the type that was more prone to fall out, and it was these lenses that Lennon likely wore.
Why did Lennon’s contact lenses usually fall out? Based on prescription in the case of the glasses he wore in 1971, Lennon not only suffered from myopia, but in addition had a moderate visual impairment astigmatism.
Astigmatism is an imperfection in the curvature of the cornea, in Lennon’s case resembling the curve of a rugby ball lying on its side. And it was Lennon’s astigmatism that most certainly led to his frequent lack of contact lenses.
ThenManufacturers have typically not modified the shape of the back surface of the contact lens to accommodate the shape of the cornea of an individual with astigmatism.
So, when a typical rigid lens is fitted to a cornea corresponding to the Lennon cornea, the lens is unstable and slides down when someone lifts the upper eyelid. It can then make a ringing sound in the eye.
Timeline Artist/Shutterstock
What does marijuana should do with it?
Lennon realized there was one thing he could do to maintain his contact lenses. According to an interview with an optometrist, Lennon he said:
I attempted to place them on, but the only method to keep them in my bloody eyes was to first get drunk on the bloody habit.
How can smoking marijuana help with wearing contact lenses?
This probably caused his upper eyelids to droop (generally known as prolapse). We do not know exactly what the connection is between cannabis and eyelid position. But a number of animal experiments
There have been reports of ptosis related to marijuana. Marijuana may reduce the function of the levator palpebrae superioris muscle, which lifts the upper eyelid.
So when Lennon was under the influence of medicine, his lowered eyelids helped keep the upper a part of the lens in place.
Lennon wore contact lenses from late 1963 to late 1966. This coincides with the peak period of The Beatles’ marijuana use. For example, Lennon refers to their 1965 album Rubber Soul as “pot album”.

Share
Back to glasses
Eventually, in 1967, Lennon stopped wearing contact lenses because they fitted poorly and began wearing glasses in public.
His frustrating experiences with contact lenses can have influenced the genesis of his iconic bespectacled look, which is still immediately recognizable greater than half a century later.